What Autism Teaches Us About Design



If people who own, operate and design buildings are not thinking about people with autism, they will be soon. Individuals diagnosed with Autism Spectrum Disorder, or ASD have the same rights to functional, accessible spaces that the non-ASD world enjoys. Also, with 1 in 68 children diagnosed with autism in 2012 — up from 1 in 150 in 2000 (See Figure 1) — it is time for the United States to expand its idea of accessibility.
Unfortunately, creating responsive buildings for people with ASD is difficult. Most architects, engineers, and building owners have limited knowledge of ASD. Its broad range in sensitivity also means that each individual needs different qualities in their surroundings. Even with the “perfect” building design, inhabitants must be empowered to interact with and modify spaces to meet their immediate needs.
Taken all together, it is not a surprise that the design world has more progress to make regarding inclusive buildings. But there is also an up-side to the challenge; everyone benefits from the features that make a facility autism-friendly. This article highlights why a focus on occupants with ASD is a powerful approach to creating great architecture.

Autism and Buildings
Autism means not feeling relaxed. It appears to be caused by complicated genetic and environmental interactions, and there is no cure. The evidence of effective interventions is limited (Rodger et al, 2010). In fact, many view ASD as a part of natural variation in human biology, not requiring a ‘cure’ (Kapp et al., 2013). The DSM-5 lists the primary criteria as deficits in social interactions and restricted, repetitive behaviors and interests. Sensory integration deficits are a second-tier criterion. Nonetheless, most individuals with ASD do experience sensory hypersensitivity or hyposensitivity, especially in hearing and touch (Fernández-Andrés et al, 2015). Alarmingly, the prevalence of ASD is around 1 percent of the population, with more males affected than females. (Mostafa, 2008; Sanchez et al, 2011).
Architecture can address the needs of occupants with ASD. That is because buildings accommodate the needs of their occupants through spatial configuration, acoustics, lighting, temperature, air quality, furnishings and finishes. A common hypothesis in the literature is that modulating these features of the physical environment can help all occupants relax and focus.
However, interventions that only address design will be of limited value because the physical environment is intertwined with the social environment (Sanchez et al, 2011). For example, a study by Fernández-Andrés et al. (2015) found that children diagnosed with ASD experienced greater sensitivity to touch when in classroom environments than when at home. The authors proposed that the social and environmental context of the classroom made physical contact more intrusive.
Occupants not only sense the quality of their surroundings — they take part in it. In this way, achieving indoor environmental quality requires that occupants interact with their physical space. Often that also entails adapting social norms for behavior, like closing blinds or wearing short sleeves. Individual factors are fundamental to understanding the drivers of this social behavior. Two of the most important personal factors for comfortable spaces are alliesthesia and executive functions.
Alliesthesia
Alliesthesia describes how an individual’s internal state and subjective conditions can make a certain stimulus pleasing or displeasing. It is a physiological phenomenon present in all the senses that helps individuals attain what they need. For example, a glass of water is satisfying to someone who is thirsty, and a cold breeze can feel good to someone who is running (de Dear, 2011). The glass of water and cold breeze can cause displeasure to the same person if his or her internal state has changed.
Underscoring alliesthesia is the fact that humans are very sensitive to changes in the environment — much more so than absolute states. By attending to these subtle changes, the organism can discern the most beneficial environmental conditions. Some examples of these stimuli are temperature, light contrast, air quality, echo and air speed. Occupants experience pleasure as a result of changes that align with their internal states. Therefore, the phenomena is highly individual, and manifests differently as a result of cultural norms.

The pleasure associated with alliesthesia may be related to the voluntary behavior of an individual seeking homeostasis, as opposed to involuntary responses such as sweating and pupil dilation. By recognizing that different individuals can have very different needs from their surroundings at different times, engineers and architects can create high-performance spaces for all occupants.
This is relevant for building design because humans like to interact with their surroundings — both to remove uncomfortable stimuli and to create sensory pleasure. For people with ASD this is relevant because hypo- and hypersensitivity is common, and can be ameliorated through the sensory environment. This may partially explain the popularity of intensive sensory therapies, which stimulate the body in an effort to modify behavior. Sensory rooms are also popular in autism-friendly spaces because they provide a controllable environment as a retreat from overwhelming stimuli.
Occupants not only sense the quality of their surroundings — they take part in it.
Executive Functions
While alliesthesia helps explain the motivation for an individual’s interaction with the surroundings, there’s another process involved when it comes to achieving comfort. Executive functions refer to a set of cognitive skills that individuals leverage to achieve their goals over the course of a lifetime. According to Mischel & Ayduk (2002), emotional regulation and cognitive control are two foundational capacities of executive functions. In their model, executive functioning involves the interplay of emotional-based impulses from the amygdala and cognitive processing of those impulses from the hippocampus.
A room that offers inhabitants control of their surroundings creates opportunities to exercise executive function. That’s especially relevant because most individuals diagnosed with ASD exhibit deficits in executive function skills (Ozonoff et al., 1991). In fact, executive functioning is a second-order criterion used in diagnosing ASD. While executive function skills may or may not be involved in the manifestation of ASD symptoms (Sanchez et al., 2011), they are nonetheless core features of many established therapies for ASD (National Autism Center, 2015).
Some popular treatments for individuals with ASD seek to transform how the body interprets sensory information. Sensory Integration Therapy and deep pressure therapy are examples of this approach. While these intensive sensory therapies may have short-term benefits, there is little evidence of their long-term impact on behavior (Rodger et al., 2010).
Nonetheless, sensory stimulation can prove to be effective in developing cognitive regulation skills. Through spaces that afford control of stimuli, inhabitants can learn to manage sensory overload — a skill that has long-term benefits (Rodger et al., 2010). Individuals also feel a greater sense of agency when they perceive control over the physical environment (Toftum, 2010).
Through spaces that afford control of stimuli, inhabitants can learn to manage sensory overload.
Design for Options
Occupants vote with their feet. By perambulating to spaces of preference, individuals select environments that support their intended occupation while also providing comfort. However, occupants cannot always choose between multiple spaces, and sometimes, one aspect of a room is annoying while everything else is fine. This is where designers can help by providing spaces with locally controlled, culturally relevant options.
Affordance is one way to think about the diversity of possibilities a space offers to inhabitants (Kinnaer et al., 2016). What affordance looks like varies dramatically due to the breadth of the autism spectrum and the purpose of the space. Which is why specific guidelines for autism-friendly spaces offer limited value; the best advice tends to be quite general.
For example, Mostafa (2014) recommends that school design for students with ASD incorporate seven principles: acoustics; spatial sequencing; escape; compartmentalization; transition spaces; sensory zoning; and safety. Each of these principles provides general information to designers for consideration without listing prescriptive criteria. Sanchez et al. (2011) also provides a broad overview of findings regarding the physical environment and ASD behavior.
Findings
Spatial Configuration
The need for personal space varies in different cultures, and between individuals. Those with ASD may also have different needs for personal space — or proxemics (Sanchez et al., 2011). For architecture, the provision of space is a first principle that shapes floors, walls and ceilings. The resulting feeling of enclosure is fundamental to the perception of safety and control. Together with the number of people in a space, enclosure sets limits for inhabitants’ personal space. Therefore, larger spaces offer meaningful options for people with ASD in achieving comfort.

In fundamental ways, perception of space for people with and without ASD is similar. A study by Cooper et al. (2015) compared adults with and without ASD in their ability to notice changes to a virtual room. Results showed that those with ASD generally had more difficulty noticing changes, but were similarly attuned to the ways the rooms had changed. This suggests a similar mental processing of space.
Spaces with certain features can be easier to adapt to, and therefore less overwhelming for occupants with ASD. Rooms that display order and definition are more legible to autistic individuals (Kinnaer et al., 2016; Gaines et al., 2014). The best spaces also feature areas and pathways that are reconfigurable for different occupants. One-way, sequential patterns reinforce routine and improve focus. Subdividing rooms so that spaces that contain a single activity also increases learning (Mostafa, 2008). Providing storage spaces for non-relevant materials helps to further encourage focus (Gaines et al., 2014).
The human preference for contrast in scale is exemplified by the evolved human-habitat relationship described by Jay Appleton in 1975. His concept of prospect and refuge has today become a design pattern for indoor spaces that combine safe shelter with expansive views (Kellert et al., 2011). This provision is especially relevant for autism-friendly spaces that provide for a broad range of spatial needs.
The frame of perception is a driving factor in creating spaces of preference, especially in the context of social interaction. A room that feels too small could also feel too large depending on the individual or individuals in question, and what they are trying to accomplish. For example, several small groups working simultaneously in a classroom may introduce too much motion and background noise for someone with ASD to participate. Similarly, attempting individual work in a gymnasium may present too much visual distraction. Layers of spaces can offer a sense of comfort, such as a tent within a room. Importantly, when occupants have control over the organization of space, they also experience greater comfort (Sanchez et al., 2011).
There is good evidence that flexible spaces are helpful for those with ASD. In a study by Hirasawa, Fujiwara & Yamane (2009), an individual with ASD exhibited fewer repetitive behaviors when classrooms and care settings were reorganized. The researchers adjusted furniture and materials to provide intentional interactions with staff and improve the comprehensibility of task sequence. The clear organization of rooms into activity areas based on intended functions is similarly a best practice for classrooms in general (Tomlinson & Imbeau, 2010).
In wayfinding, symbols and coordinated colors or distinctive landmarks can improve navigation. This is especially true when the signals are culturally relevant and related to the intended use of the space (Mostafa, 2008; Sanchez et al., 2011). One possible explanation for this finding is that individuals with ASD are better at navigating spaces when there is a clear objective. A study by Fornasari et al. (2012) found that children with ASD explored virtual environments similarly to a control group when searching for objects in the game. However, they explored less area when instructed to explore the environment without such an objective goal.
When occupants have control over the organization of space, they also experience greater comfort.
Acoustics
Sound perception occurs in numerous ways. For indoor environments, considerations include background noise (e.g. mechanical equipment) and distracting sounds (e.g. a ringing phone). Reverberation time also relates to the perception of how ‘live’ or ‘dead’ a room feels.
Rooms may be too loud or too quiet. The ability to adjust the equivalent sound pressure level of background noise is likely an important feature of spaces for all occupants. For example, adding background noise with biophilic elements, such as birdsong or water sounds, can reduce occupants’ stress (Mackrill et al., 2014). Adding pink noise is another common strategy for creating sound privacy in spaces with diverse activities.
Sound carries messages; most notably, speech. Electro-acoustic paging systems and alarms are also examples of meaningful sounds. These encoded signals are almost always distracting and can be minimized to create the best possible space. There is considerable individual variance regarding the impact of background noise containing speech (Clausen & Wyon, 2008). It’s likely that individuals with ASD are particularly sensitive. In a study of time on-task in speech therapy rooms, autistic children maintained focus longer when the rooms were better insulated from external noise and reverberation time was decreased (Mostafa, 2008).
Lighting
In addition to rendering the world in radiant colors and shadows, light interacts with human physiology. In the ubiquitous indoor habitat, exposure to light is much lower than that outdoors. The eyes and skin serve as the body’s connection to the luminous environment. The retina is partly responsible for melatonin levels in the body, which impact mood and circadian sleep cycles. Through this mechanism, exposure to light is related to mood disorders such as depression (Srinivasan, 2006), and even the incidence of breast and prostate cancer (Stevens, 2007). Artificial lighting disrupts the light-dark environment, thereby contributing to melatonin suppression and poor sleep for individuals with ASD (Leu et al., 2011). Melatonin treatments can improve sleep for individuals with ASD (Reiter et al., 2009).
Light also has a psychological dimension. For example, colors impact mood and behavior. Occupants exhibit greater creativity in the presence of green and blue, and red may undermine cognitive performance (Eliot & Maier, 2014; Gaines et al., 2014). Autism-friendly designs generally incorporate unsaturated, light earth tones with only small, contained areas of bright color (Mostafa, 2014).
Sunlight exposure is associated with Vitamin D, which functions to help repair DNA damage (Kinney et al., 2010). Therefore, parents who are Vitamin-D deficient experience greater likelihood of having children with ASD. For community health, facilities can provide access to sunlight — both through quality daylight design indoors and by making outdoor spaces available to inhabitants.
Thermal Comfort
Heat transfer between the human body and its surroundings entails the most intimate measure of quality in the physical environment. This is because heat has an important psychological dimension that forms in the first hours of life and continues to impact perceptions and interactions. For example, Bargh & Shalev (2012) found that experiences of physical warmth increased feelings of social warmth in college students, suggesting that individuals seek physical warmth in ways similar to their desire for experiences of social warmth.

Thermal comfort depends in part on air temperature and air velocity. Building designers and operators can provide opportunities for alliesthesia to occupants by modulating these variables. Because there is no evidence relating thermal comfort to ASD, generalizations are necessary. Strategies for improving comfort include varying temperature set points for different spaces, providing ceiling fans, providing operable windows and giving occupants control of these amenities.
Materials
Finishes and furniture represent a small portion of most construction budgets, but have a big impact on indoor environmental quality. Bookshelves, workstations and seating are examples of furnishings that define the size and privacy of spaces. Because of the importance of these dimensions for people with ASD, movable furniture is better than built-in furniture. This is especially true when it can reinforce the social use of space by groups or individuals (Gaines et al., 2014; Sanchez et al., 2011).
Furnishings, carpet and wall finishes also introduce chemicals into spaces that may jeopardize the health of future parents. For example, the flame retardants used in most furniture and electronics increase the risk of having children with ASD (Messer, 2010). Larsson et al. (2009) also found that the type of flooring in parents’ bedroom was associated with the incidence of ASD in their children. Children with parents who experience elevated exposure to common mutagens such as mercury, cadmium and vinyl chloride have greater risk of ASD (Kinney et al., 2010).
Air Quality
Scientific knowledge on the impact of air pollution on health is far from complete. The evidence that does exist is vital for the operation of buildings, which can clean the outdoor air for occupants. However, even this measure does not obviate the need for awareness of air pollution in urban environments, especially for expecting mothers.
The risk of having a child with autism is greater for mothers who live near traffic sources of pollutions. A study of children diagnosed with ASD in Los Angeles between 1998 and 2009 showed that their mothers experienced elevated levels of ozone, respirable particulate matter, and nitric oxide (Becerra et al., 2013). Parents who live near power plants with mercury emissions are more likely to have autistic children, as are those in urban environments in general (Kinney et al., 2010).
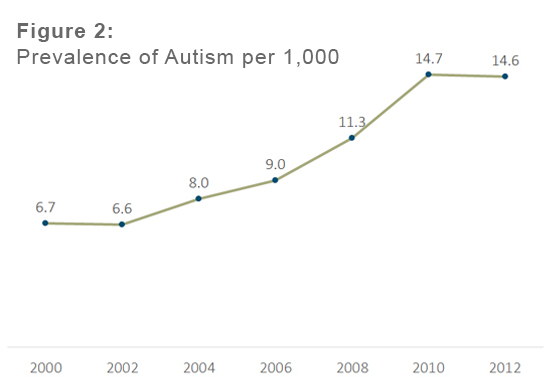
Reinforcing these findings, a recent nation-wide study of mothers (n=1,767) found that exposure to respirable particulate matter (PM2.5) during pregnancy increased the odds of having a child with ASD by 57 percent (Raz et al., 2015). It appears that exposure to this common product of motor vehicles may be most detrimental during the third trimester of pregnancy. Regarding the general risk of living in the city, a study of children in Denmark (Laurtisen et al., 2014) shows that the prevalence of ASD increases with population density. Data from this article is depicted in Figure 2.
Thankfully, buildings are able to remove particulate matter and ozone using specialized MERV 13 and activated carbon filters. However, buildings also have the challenge of managing contaminants that are released from within the space. Common indoor contaminants are cleaners, food, plants, electronic equipment and people. Using either dilution, displacement, or a combination of both, building designers attempt to deliver ‘fresh’ air to the breathing zone. This practice is called ventilation.
There is not yet evidence on ventilation for individuals with ASD. Air quality research may be generalizable to individuals with ASD. A study by Allen et al. (2016) with 24 subjects correlated cognitive functioning with increased air quality. Specifically, CO2, volatile organic compounds and ventilation rate explained over 80% of the observed increase in human performance.
Following the protocol of the Allen et al. study, a best practice for autism-friendly architecture is to provide 40 cubic feet per minute of fresh air per person. Another best practice is to provide ultraviolet lamps (ultraviolet germicidal irradiation) in air handlers to reducing the spread of illness within buildings.
The presence of perceived risk and peril in the built environment may impact behavior for individuals with ASD, although there is currently no research in this area.
Safety
Because behavior for individuals with ASD can be unpredictable, a robust physical environment is desirable. Appropriate levels of risk can be incorporated into spaces while eliminating likely hazards. For example, regulating water temperatures is an important precaution for occupants who register temperature slowly (Sanchez et al., 2011). Anchoring larger, unstable furnishings and providing resilient surfaces can reduce hazards. Designers who avoid features with sharp corners will eliminate the need for corner protection, thereby reducing visual clutter.
Autism-friendly designs generally incorporate unsaturated, light earth tones with only small, contained areas of bright color.
Role of the Design Team
Understanding how groups interact is key to designing comfortable spaces. Individuals share goals, values and experiences together that create norms of interaction. They also participate in a larger community context to produce cultural capital. For these reasons, an ethnographer can help interpret and define the architectural requirements to help align the building with its purpose. This approach uses observations, in-context interviews and surveys to better understand social interactions.
Making great spaces for all inhabitants may not be easy, but it doesn’t have to cost a fortune. Many of the design interventions described here represent a small premium on initial construction cost, and may be easily retrofitted for existing buildings. A universal design approach requires planning for increased floor area and additional consultation with experts. Importantly, explicit input from building users may be the design team’s best strategy for a successful result (McAllister & Maguire, 2012).
Buildings for Everyone
School policy regarding specific groups can catalyze larger social discussions about equity; including students diagnosed with ASD in general classrooms is a challenging mandate, and it necessitates an individualized approach. However, it is clear that physical spaces that work well for students with ASD are also great for everyone. If autism-friendly classrooms are even a minor aid in achieving a more inclusive school culture, the incremental cost would be efficacious.
There is suggestive evidence that the physical environment can benefit individuals with ASD. Sizing spaces appropriately for the intended activity is vital. Acoustics, lighting, air quality, thermal comfort, and safety add a layer of quality that further improves occupant health and comfort for individuals with ASD.
However, this overview also shows that the same strategies can make spaces more enjoyable for neurotypical individuals. In other words, autism-friendly design is just good architecture. Indeed, each student, employee and customer has needs of their environment that can only be standardized at the expense of accommodation. Recognizing and enacting this mandate for flexible, comfortable spaces is an opportunity we can explore together.
Additional Resources:
Usability Principles to consider when designing or renovating a space – Download
Sources:
Allen, J. G., MacNaughton, P., Satish, U., Santanam, S., Vallarino, J., & Spengler, J. D. (2016). Associations of cognitive function scores with carbon dioxide, ventilation, and volatile organic compound exposures in office workers: a controlled exposure study of green and conventional office environments. Environmental Health Perspectives, 124(6), 805.
Bargh, J. A., & Shalev, I. (2012). The substitutability of physical and social warmth in daily life. Emotion, 12(1), 154.
Becerra, T. A., Wilhelm, M., Olsen, J., Cockburn, M., & Ritz, B. (2013). Ambient air pollution and autism in Los Angeles County, California. Environmental Health Perspectives (Online), 121(3), 380.
Christensen, D. L. (2016). Prevalence and characteristics of autism spectrum disorder among children aged 8 years–autism and developmental disabilities monitoring network, 11 sites, United States, 2012. MMWR Surveillance Summaries, 65 (No. SS-3):1—23.
Clausen, G., & Wyon, D. P. (2008). The combined effects of many different indoor environmental factors on acceptability and office work performance. HVAC&R Research, 14, 103-113.
Cooper, R. A., Plaisted-Grant, K. C., Hannula, D. E., Ranganath, C., Baron-Cohen, S., & Simons, J. S. (2015). Impaired recollection of visual scene details in adults with autism spectrum conditions. Journal of abnormal psychology, 124(3), 565.
De Dear, R. (2011). Revisiting an old hypothesis of human thermal perception: alliesthesia. Building Research & Information, 39(2), 108-117.
Elliot, A. J., & Maier, M. A. (2014). Color psychology: effects of perceiving color on psychological functioning in humans. Annual review of psychology, 65, 95.
Fernández-Andrés, M. I., Pastor-Cerezuela, G., Sanz-Cervera, P., & Tárraga-Mínguez, R. (2015). A comparative study of sensory processing in children with and without autism spectrum disorder in the home and classroom environments. Research in developmental disabilities, 38, 202-212.
Fornasari, L., Chittaro, L., Ieronutti, L., Cottini, L., Dassi, S., Cremaschi, S., Molteni, M., Fabbro, F. & Brambilla, P. (2013). Navigation and exploration of an urban virtual environment by children with autism spectrum disorder compared to children with typical development. Research in Autism Spectrum Disorders, 7(8), 956-965.
Gaines, K. S., Curry, Z., Shroyer, J., Amor, C., & Lock, R.H. (2014). The perceived effects of visual design and features on students with autism spectrum disorder. Journal of Architectural and Planning Research, 31(4), 282-298.
Hirasawa, N., Fujiwara, Y., & Yamane, M. (2009). Physical arrangements and staff implementation of function-based interventions in school and community settings. Japanese Journal of Special Education, 46(6), 435-446.
Kapp, S. K., Gillespie-Lynch, K., Sherman, L. E., & Hutman, T. (2013). Deficit, difference, or both? Autism and neurodiversity. Developmental Psychology,49(1), 59.
Kellert, S. R., Heerwagen, J., & Mador, M. (2011). Biophilic design: the theory, science and practice of bringing buildings to life. John Wiley & Sons.
Kinnaer, M., Baumers, S., & Heylighen, A. (2016). Autism-friendly architecture from the outside in and the inside out: An explorative study based on autobiographies of autistic people. Journal of Housing and the Built Environment, 31(2), 179-195.
Kinney, D. K., Barch, D. H., Chayka, B., Napoleon, S., & Munir, K. M. (2010). Environmental risk factors for autism: do they help cause de novo genetic mutations that contribute to the disorder? Medical hypotheses, 74(1), 102-106.
Larsson, M., Weiss, B., Janson, S., Sundell, J., & Bornehag, C. G. (2009). Associations between indoor environmental factors and parental-reported autistic spectrum disorders in children 6—8 years of age. Neurotoxicology,30(5), 822-831.
Leu, R. M., Beyderman, L., Botzolakis, E. J., Surdyka,K., Wang, L., & Malow, B. A. (2011). Relation of melatonin to sleep architecture in children with autism. Journal of autism and developmental disorders, 41(4), 427-433.
Mackrill, J., Jennings, P., & Cain, R. (2014). Exploring positive hospital ward soundscape interventions. Applied ergonomics, 45(6), 1454-1460.
Martin, C. S. (2014). Exploring the impact of the design of the physical classroom environment on young children with autism spectrum disorder (ASD). Journal of Research in Special Educational Needs.
McAllister, K., & Maguire, B. (2012). A design model: The autism spectrum disorder classroom design kit. British Journal of Special Education, 39(4), 201-208.
Messer, A. (2010). Mini-review: polybrominated diphenyl ether (PBDE) flame retardants as potential autism risk factors. Physiology & behavior, 100(3), 245-249.
Mischel, W., & Ayduk, O. (2002). Self-Regulation in a Cognitive--Affective Personality System: Attentional Control in the Service of the Self. Self and Identity, 1(2), 113-120.
Mostafa, M. (2008). An architecture for autism: Concepts of design intervention for the autistic user. Archnet-IJAR: International Journal of Architectural Research, 2(1), 189-211.
Mostafa, M. (2014). Architecture for autism: autism ASPECTSS™ in school design. International Journal of Architectural Research, 8(1), 143-158.
National Autism Center. (2015). Findings and conclusions: National standards project, phase 2. Randolph, MA.
Ozonoff, S., Pennington, B. F., & Rogers, S. J. (1991). Executive function deficits in high-functioning autistic individuals: relationship to theory of mind. Journal of child Psychology and Psychiatry, 32(7), 1081-1105.
Raz, R., Roberts, A. L., Lyall, K., Hart, J. E., Just, A. C., Laden, F., & Weisskopf, M. G. (2015). Autism spectrum disorder and particulate matter air pollution before, during, and after pregnancy: a nested case—control analysis within the Nurses’ Health Study II cohort. Environmental Health Perspectives, 123(3).
Reiter, R. J., Tan, D. X., Erren, T. C., Fuentes-Broto, L., & Paredes, S. D. (2009). Light-mediated perturbations of circadian timing and cancer risk: a mechanistic analysis. Integrative Cancer Therapies, 8(4), 354-360
View More Resources
Benefit from our expertise

